

When you first make a decision to start TRT, or testosterone replacement therapy, one popular drug will always crop up in discussions, Sustanon 250.
This drug has the ability to evoke strong opinions, many men swear by it while others absolutely hate it. You would think that they were discussing Marmite. What is it about Sustanon 250 that causes such strong views? In this blog we will attempt to objectively study Sustanon to provide you with a balanced view to help you decide if this is the best TRT option for you.
-
 Sildenafil 100mg Tablets£9.99 – £31.99
Sildenafil 100mg Tablets£9.99 – £31.99 -
 Sildenafil 50mg Tablets£7.99 – £31.99
Sildenafil 50mg Tablets£7.99 – £31.99 -
 Sildenafil 25mg Tablets£5.99 – £21.99
Sildenafil 25mg Tablets£5.99 – £21.99
What is Sustanon?
Sustanon 250 is an oil based (arachis or peanut oil) injectable testosterone blend of four testosterone esters which have been modified by the addition of carboxylic acid esters (propionic, propionic phenyl ester, isocaproic and decanoic acids) at the 17- beta hydroxyl position.
What does Sustanon 250 contain?
Sustanon 250 contains the following:
- Testosterone propionate 30mg
- Testosterone phenyl propionate 60mg
- Testosterone isocaproate 60mg
- Testosterone decanoate 100mg
What form does Sustanon come in?
Sustanon 250 is available in 1ml ampules which contain 176mg of testosterone.
How is Sustanon 250 administered?
Sustanon 250 is administered by intramuscular injections
Why does Sustanon 250 have to be given by injection?
Sustanon 250 is given by intramuscular injection due to the fact that if it is taken orally it it will be subject to extensive first pass metabolism by the liver.
Orally administered unmodified testosterone has a short half-life and poor bioavailability, because it is readily metabolized in the liver. Testosterone is therefore chemically altered to produce clinically useful preparations.
In Sustanon 250 the testosterone molecule has esters with differing side chains added to it. This chemical modification slows down the rate of absorption and breakdown and facilitates maintenance of therapeutically effective testosterone levels.
Is Sustanon 250 legal in the UK?
Sustanon 250 is a popular form of TRT that is readily available via the legal pharmaceutical chain in the UK. It is listed in the BNF, that is the British National Formulary, and can be obtained against both an NHS and a private prescription.
Is Sustanon available in the UK?
Sustanon 250 is available from the two largest UK pharmaceutical wholesalers, AAH and Alliance Healthcare. It is readily available but does tend to go out of stock, so it is best to ensure that the pharmacy you choose to collect from has adequate supplies.
History of Sustanon
Sustanon 250 made its first appearance in the 1970s. It was developed by the pharmaceutical company Organon which is now known as Merck/MSD. However, the pharmaceutical company Aspen based in Ireland now manufactures the Sustanon 250 for UK supply.
Is Sustanon 250 a “stack”?
In terms of “bro science” Sustanon 250 is a “stack”. What this means is that Sustanon 250 is a combination of four different testosterone esters that together produce an extended release profile. This means fewer intramuscular injections are required so you don’t have to transform your body into a pin cushion.

What are Testosterone esters?
The four testosterone esters contained in Sustanon 250 each have different durations of action. An ester is a chemical compound with the following general chemical structure.
Structure of an ester

If you know your chemistry then you will recognise this structure but don’t worry if you don’t. All you need to know is that when esters are added to the testosterone molecule it has the effect of making it more lipophilic, or more soluble in fat or oil. This is an important property of the testosterone esters which will be covered in more detail further on.
To help understand what goes on when Sustanon 250 is injected into the body it is helpful to study the structural formula of a testosterone molecule. Brace yourself for a flashback to your school chemistry lessons.
Structural formula of testosterone
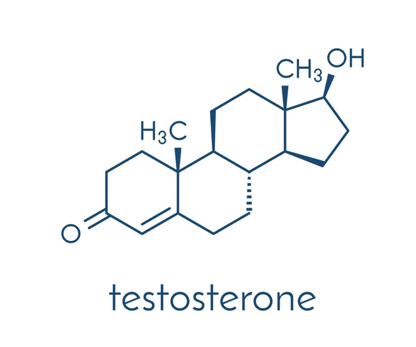
This is the structural formula for testosterone. Chemists, being the nerds, they are, like to be precise and so they like to give each carbon atom a number. When we number the above molecule, we get the following:
Numbering of the testosterone molecule
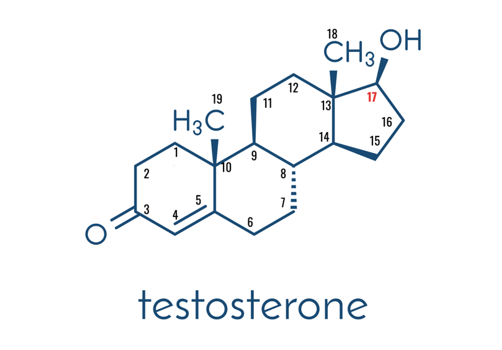
So, when fully labelled we can count the number of carbon atoms in the testosterone molecule; there are 19. From the point of view of the testosterone esters in Sustanon 250, the most important carbon atom is in position 17. Carbon number 17 on the testosterone molecule is where the secret sauce is added.
Now that the testosterone molecule has made it introduction, it’s time to look at the four different testosterone esters in Sustanon 250.
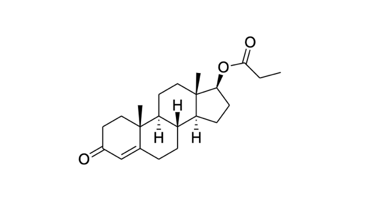
Testosterone Propionate
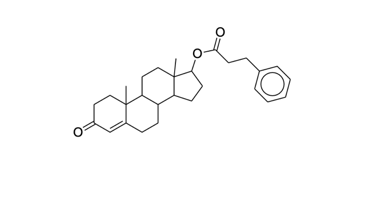
Testosterone Phenylpropionate
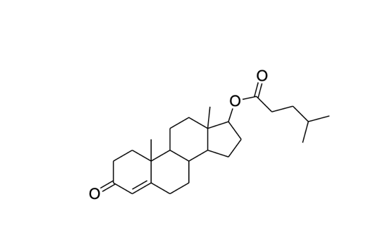
Testosterone Isocaproate
Testosterone Decanoate
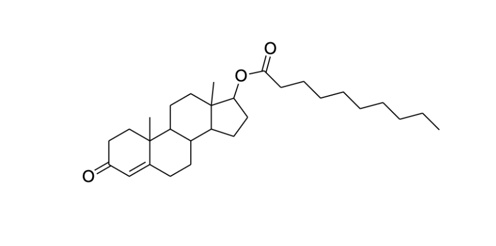
You don’t need to have a PhD in chemistry to see that the carbon chain added at position 17 gets progressively longer.
The shortest chain being testosterone propionate and the longest decanoate. Want to know why it’s called decanoate? Because there are 10 carbon (deca) atoms in the chain.
The theory behind Sustanon 250
Sustanon is designed to provide an initial rapid increase in testosterone levels followed by a more extended release profile. This is based on the different release characteristics of the testosterone esters.
The rationale behind the use of testosterone esters is to prolong the therapeutic window following administration, which will lead to fewer injections compared to unesterified steroid injections.
In these preparations, testosterone is esterified at the 17-hydroxy position (see above diagram). This modification of the molecule decreases the polarity (less water loving) making it more lipophilic (fat loving), thus making the molecule more soluble in the injection oil. This has the effect of slowing down the absorption of testosterone from the area of injection. Once in the bloodstream, the ester is removed (hydrolysed – see below) to release the free or active testosterone into the circulation, thereby creating a long-acting effect.[1]
The testosterone esters in Sustanon 250 each have different pharmacokinetic profiles and elimination release half-lives. Thus, each testosterone ester will diffuse into the blood in sequence of increasing lipophilicity. This will, in effect, cause a steady state of normalised testosterone levels.
Sustanon 250 was designed to provide a more physiologic like testosterone levels compared when the individual testosterone esters are used individually.
So, when the testosterone propionate has been eliminated then the testosterone phenylpropionate would kick in, and so on. Sequential diffusion of the esters from the area of injection would in theory facilitate steady state levels of testosterone.
Sequential Release of Testosterone Esters

This seems good in theory ,however, in practice it doesn’t quite work out this way. Studies have shown that these preparations are actually more likely to cause a higher initial supraphysiologic (above normal) peak in testosterone levels. That means that there is significant overlap between the esters. This will be discussed in further details below when we will analyse the pharmacokinetic release studies on Sustanon 250.
Is Sustanon a “prodrug”?
You can think of Sustanon, or any testosterone ester for that matter, as a kind of “prodrug”. This is a drug which is only activated once the body performs an enzymatic action on it. In the case of Sustanon 250 and other testosterone esters it is a process called hydrolysis carried out by blood esterase enzymes.
Hydrolysis of testosterone esters
Once in circulation, hydrolysis rapidly occurs by the action of blood esterase’s to yield the active compound. Hydrolysing esters involves splitting them into carboxylic acids (or their salts) and alcohols by the action of water, dilute acid or dilute alkali.
Once the testosterone esters in Sustanon 250 have been hydrolysed, the testosterone is released and can then enter the general circulation. From the circulation it can travel around the body to act on the androgen receptor (AR) inside cells.
The unesterified testosterone, therefore, is the active substance for testosterone substitution therapy of male hypogonadism
Hydrolysis of testosterone decanoate

This completes the brief introduction into the basic chemistry and pharmacokinetic profile of Sustanon 250. We will now delve more deeply into the controversial pharmacokinetic profile of Sustanon 250 and discover how theory does not always work the way we would like in the real world.
Pharmacokinetics of Sustanon 250
The term pharmacokinetics refers to how the body acts on the drug in terms of administration, distribution, metabolism and excretion. This is summarised by the acronym ADME.
So, while pharmacokinetics describes how the body processes the drug, pharmacodynamics refers to the action the drug does to the body.
It is important to have a good understanding of a drug’s pharmacokinetic profile since this will allows the drug’s dosing regimen to be calculated.
Absorption
A single dose of Sustanon 250 leads to an increase of total plasma testosterone with peak levels of approximately 70nmol/l, which are reached approximately 24-48 h after administration. Plasma testosterone levels return to the lower limit of the normal range in males in approximately 21 days.
Distribution
After hydrolysis of the testosterone esters the testosterone enters circulation in the plasma, or blood, where it hitches a ride on carrier proteins such as albumin and SHBG.
Under physiological conditions, approximately 70% of testosterone is bound to SHBG with high affinity, while about 20–30% is weakly bound to albumin, with the remaining 1-2% being free.[2]
This means that only about 1-2% of testosterone is “free” and able to exert its action on the androgen receptor inside cells.
Metabolism
Testosterone is metabolised to dihydrotestosterone via 5 alpha reductase and oestradiol via the aromatase enzyme, which is found in adipose or fat tissue.
Elimination
Excretion mainly takes place via the urine as conjugates of etiocholanolone and androsterone.
Testosterone is metabolised predominantly in the liver and converted by 17?-hydroxy dehydrogenase into androsterone and etiocholanolone, which are biologically inactive.
DHT is metabolised to androsterone, androstenedione and androstenediol.
These compounds then undergo the chemical processes of glucuronidation or sulfation which basically makes molecules more polar and hence easier to excrete in the urine.
Summary of pharmacokinetics of Sustanon 250
So, from the pharmacokinetic profile the data suggest that Sustanon 250 will provide a physiological level of testosterone for up to 21 days. This is in fact confirmed by studies on the pharmacokinetic profile of Sustanon 250 that found that it provided a rapid peak in testosterone levels (24-48 Hours after injection) and maintained physiological concentrations for approximately 21 days.[3]
Esterification of the testosterone molecule at position 17, e.g., with propionic or enanthic acid, prolongs the activity of testosterone in proportion to the length of the side chain when administered intramuscularly (Junkmann 1952, 1957).[4]
Comparisons of the absorption kinetics of different testosterone esters clearly show that the half-lives of the absorption of the esters increase when the esterified fatty acids have a longer chain (van der Vies 1985).[5]
So, the longer the side chain at position 17, the longer the duration of action of the testosterone ester. This is exploited in Sustanon 250 with each ester having a progressively longer chain. So, in theory when the shorter ester chains are being eliminated the intermediate esters are in the process of being absorbed.
Studies were able to show that after intramuscular administration, the testosterone ester is slowly absorbed into the general circulation and then rapidly converted to the active unesterified metabolite (Fujioka et al. 1986).[6]
The observation that the time at the injection site is the major factor determining the residence time of the drug in the body agrees with pharmacokinetic studies which demonstrated that the testosterone ester is absorbed unchanged from the injection depot in the muscle into the general circulation according to first-order kinetics, that is the rate of elimination of the drug is proportional to its concentration, with a long half-life ( time taken for the drug to reduce to half of its original concentration) of 130 h (van der Vies 1965)[7]
The ester is then rapidly hydrolysed in plasma, as could be shown by in vitro rat studies (van der Vies 1970)[8] and in vivo human studies (Fujioka et al. 1986)[9].
Although the rate of hydrolysis again depends to some degree on the structure of the acid chain, this process in comparison to the release from the injection deposit, is far more rapid (van der Vies 1985).
So, the main determining factor effecting the activity of testosterone esters is absorption of the testosterone ester from the site of administration into the plasma. This is because in comparison the process of hydrolysis of the esters is rapid.
Further proof of the rapid hydrolysis of the testosterone esters to the unesterified testosterone have been confirmed by studies which injected both testosterone and testosterone enanthate intravenously. If there was a delay in the hydrolysis of testosterone enanthate then this would be reflected in a different pharmacokinetic profile. However, after intravenous injection of testosterone enanthate or testosterone these compounds have similar pharmacokinetics (Sokol and Swerdloff 1986)[10]

Based on this assumption it is easier to calculate the pharmacokinetic profiles of different testosterone esters by simply measuring the unesterified testosterone. It is also possible to measure the ester levels in the blood, but it is more complicated and is mainly reserved for testing for doping in sports. (Cantrill et al. 1984)[11] However, this is based on an important assumption regarding testosterone levels in hypogonadal men.
It is known from clinical studies for male contraception that testosterone esters suppress the endogenous lutenising hormone (LH) and testosterone secretion (Nieschlag and Behre 1997)[12]. If pharmacokinetics of testosterone esters are studied in normal male volunteers, the testosterone concentration measurable in the serum is the sum of the endogenous (produced by the body) testosterone and the exogenous (supplied from outside the body) testosterone hydrolysed from the ester (Anderson et al. 1997).[13]
Because the endogenous testosterone is suppressed to hypogonadal values during the first days after administration of the testosterone ester, the changes in testosterone serum concentrations after administration represent the combined pharmacokinetics of the endogenous and exogenous testosterone.
Hypogonadal patients are characterised by impaired or absent endogenous testosterone secretion; exogenous testosterone administration can further suppress endogenous testosterone secretion only to a limited degree, if at all. Accordingly, in hypogonadal patients the serum concentration versus time profile is mainly a reflection of the pharmacokinetics of the exogenously administered testosterone ester alone.
Detection of testosterone esters in blood plasma for doping
Despite the rapid hydrolysis of the testosterone esters in the serum it is still possible to measure the concentration of the esters themselves. However, this requires a greater degree of sophistication and this method is used when testing for performance enhancing drugs in sport.
When testosterone ester preparations are applied, either orally or as a depot injection, the ester diffuses slowly into the bloodstream. Although the cleavage process, by esterase enzymes starts immediately, a detectable portion of the pro-drug, the testosterone ester itself, is still detectable in the blood.[14] Since these testosterone esters are not produced naturally by the body, when they are detected in the plasma it provides proof of doping if they are used to gain an unfair advantage in profession sports.
A clinical study was designed to investigate the detection window of injected testosterone esters as a mixed substance preparation (Sustanon) and as a single substance preparation in serum and plasma. The study comprised of six participants who were either administered a single intramuscular injection of either 1000mg testosterone undecanoate (Neida) or a Sustanon. Blood samples were taken regularly throughput a testing period of 60 days and the analytical methods for blood analysis employed liquid chromatography-tandem -mass-spectrometry (LC-MS/MS). It was found that all testosterone esters could be subsequently detected in the samples.[15]
The results of this study found that the depot effect of the testosterone ester preparation increases in proportion to the length of the ester side chain. This is because the half-life of the absorption increases with longer chains.[16] Hence, the different testosterone esters do not have the same terminal half-lives, and the elimination of testosterone esters, administered intramuscularly is suggested to be absorption rate limited. This is because once the testosterone esters have managed to diffuse into the plasma from the depot the hydrolysis occurs at a rapid rate.
The following graphs illustrate the findings. As expected, the shortest chained ester, testosterone propionate showed the most rapid elimination and shortest half-life. However, the ester could still be detected for at least 4 days in serum and plasma of all study participants receiving the drug.
Elimination of testosterone propionate

Elimination of testosterone phenylpropionate

Elimination of testosterone isocaproate

Elimination of testosterone decanoate

For testosterone phenylpropionate and testosterone isocaproate similar pharmacokinetic profiles were observed, with respect to half-lives as well as detection times in the blood. The half-lives were estimated to 2.5 and 3.1 days, respectively. Both esters were detected for at least 8 days in all study subjects. The longest detection time observed was 11 days (Subjects 1 and 3).
Regarding the long-chained ester testosterone decanoate, the compound was found to have a detection time of 18 days. Hence, the duration of detection was markedly longer compared to the shorter chained esters testosterone propionate, testosterone phenylpropionate and testosterone isocaproate. The terminal half-life of testosterone decanoate was estimated to be 5.6 days.
Testosterone concentrations after administration of Sustanon
The testosterone levels achieved after the administration of Sustanon was studied by Cantrill Ja et al.[17] Hormone responses to Sustanon were studied in 9 hypogonadal males. It was found that serum testosterone rose to supraphysiological peak concentrations ( mean 71mol/L) 24-48 hours after an injection, followed by an exponential decay to reach baseline concentrations after 2-3 weeks. The overall calculated mean testosterone level in subjects receiving Sustanon 250 every three weeks was 27.7nmol/L.
Testosterone concentrations obtained from patients while on Sustanon 250 injection are shown in the following graph.

The peak concentration obtained ranged from 42-121 nmol/k (mean 71nmol/L) and occurred 24-48h after the injection. The mean concentration fell to within the normal male range after one week and fell to the lower limit of the normal male range after 21 days. The overall mean testosterone level was 27.7nmol/L. It was also found that the administration of Sustanon 250 produce consistently higher peak metabolite concentrations when compared to testosterone undecanoate and testosterone implants. Peak 3 alpha-diol and DHT concentrations were only just outside the normal male range, but those of E2 were twice the upper limit of normal.
Intramuscular injections of Sustanon 250 was found to produce supraphysiological levels of both testosterone and oestradiol soon after injecting persisting for up to days, with peak concentrations occurring within 24-48h. Two patients in the study experienced breast tenderness in the first few days following injection which may be attributed to higher E2 concentrations. Similarly, two patients reported increased aggression after their injections. However, overall this study reported a good clinical response in all subjects.
Sustanon conclusion
So, there you have it. An extensive analysis of the pharmacokinetic profile of Sustanon 250. As you can see the studies have demonstrated that the esters combine initially to produce a supraphysiological peak. However, one can question this phenomenon due to the fact that we are not told the baseline testosterone levels of the participants.
As was touched upon earlier it takes time for the exogenous Sustanon 250 to turn off the LH/FSH pathway and so when Sustanon 250 is initially administered the two testosterone levels are combined. This would then imply that once the hypothalamus-pituitary-gonadal axis is switched off subsequent Sustanon 250 injections will remain within normal limits.
This ability to critically analyse scientific papers is absolutely vital to make sure that no one is trying to pull the wool over your eyes. Different parties have vested interests, so it takes a bit of elbow grease and common sense to arrive at an accurate interpretation of the paper.
With regards to the dosing of Sustanon 250 the studies are in agreement that the physiological testosterone levels remain in the body for about 21 days. However, this does not mean that every man should be given one Sustanon 250 injection every three weeks. Every man is different, complete with their own genetic make-up. Their reaction enzymes may be present in different quantities thus affecting the speed of processes within the body. So, what may be a suitable dosing regimen in one man may not be sufficient in another who may require more frequent injections.
This is the nub of the issue, TRT should be tailored to the individual. It is not a one size fits all model. Find a TRT clinics which treats the person and not the numbers.
We understand that everyone is different and will react to TRT in different ways. Differences at the genetic level influence how men will respond to TRT. For example, the differing number of CAG repeats found on the androgen receptor profoundly influence the response to testosterone replacement therapy. This itself is an exciting area of research which will hopefully lead, one day, to a pharmacogentic solution to TRT. That is the TRT will be bespoke to your genetic profile. Until that day comes try to work with a TRT expert who will work with you, factoring in all the differentials to arrive at a tailored testosterone replacement therapy solution.
If you are concerned about low testosterone, or even to find out more, please contact us for a FREE consultation.
Disclaimer: This information is for educational purposes only and not a substitute for professional medical advice.
Are weight loss treatments making you tired, or have they led to a sudden increase in hair loss? Do you struggle with sleep?
Get a free month’s supply of one of our compounded treatments for energy, hair loss or sleep, with your first purchase of Mounjaro or Wegovy from Medical Mojo.
Claim your FREE offer
References:
[1] U. Srinivas -Shankar, F.C Wu. Drug insight: testosterone preparations. Nat Clin. Prac. Urol. 2006, 3, 65
[2] Dunn J. F., Nisula B. C., Rodbard D. Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. Journal of Clinical Endocrinology and Metabolism. 1981;53(1):58–68. doi: 10.1210/jcem-53-1-58.
[3] Product Data Sheet: Sustanon 250. August 31, 2001. Pharmaco (N.Z) Ltd Auckland New Zealand
[4]Junkmann K (1957) Long-acting steroids in reproduction. Recent Prog Horm Res 13:389- 419
[5] van der Vies J (1985) Implications of basic pharmacology in the therapy with esters of nan- drolone. In: Eikelboom FA, van der Vies J (eds) Anabolics in the ’80s. Acta endocrinol, suppl 271, 110:38-44
[6] Fujioka M, Shinohara Y, Baba S, Irie M, Inoue K (1986) Pharmacokinetic properties of testosterone propionate in normal men. J Clin Endocrinol Metab 63:1361-1364
[7] van der Vies J (1965) On the mechanism of action of nandrolone phenylpropionate and nandrolone decanoate in rats. Acta endocrinol 49:271-282
[8] van der Vies J (1970) Model studies in vitro with long-acting hormonal preparations. Acta endocrinol 64:656-669
[9] Fujioka M, Shinohara Y, Baba S, Irie M, Inoue K (1986) Pharmacokinetic properties of testosterone propionate in normal men. J Clin Endocrinol Metab 63:1361-1364
[10] Behre H.M., Oberpenning F., Nieschlag E. (1990) Comparative pharmacokinetics of androgen preparations: Application of computer analysis and simulation. In: Nieschlag E., Behre H.M. (eds) Testosterone. Springer, Berlin, Heidelberg.
[11] CANTRILL, J.A., DEWIS, P., LARGE, D.M., NEWMAN, M. and ANDERSON, D.C. (1984), WHICH TESTOSTERONE REPLACEMENT THERAPY?. Clinical Endocrinology, 21: 97-107.
[12] Nieschlag E, Behre HM (1997) Male contribution to contraception – experimental approaches. In: Nieschlag E, Behre HM (eds) Andrology – Male reproductive health and dysfunction. Berlin, Heidelberg, New York: Springer-Verlag, pp 386-393
[13] Anderson RA, Wallace AM, Kiernan AT, Wu FC (1997) Comparison between testosterone en- anthate-induced azoospermia and oligozoospermia in a male contraceptive study. IV. Sup- pression of endogenous testicular and adrenal androgens. Hum Reprod 128:1657-1662
[14] de la Torre, X., Segura, J., Polettini, A. and Montagna, M. (1995), Detection of testosterone esters in human plasma. J. Mass Spectrom., 30: 1393-1404.
[15]Forsdahl G, Erceg D, Geisendorfer T, et al. Detection of testosterone esters in blood. Drug
Test Anal. 2015;7(11-12):983-989.
[16] van der Vies J. Implications of basic pharmacology in the therapy with esters of nandrolone. Acta Endocrinol Suppl (Copenh). 1985;271:38-44
[17] CANTRILL, J.A., DEWIS, P., LARGE, D.M., NEWMAN, M. and ANDERSON, D.C. (1984), WHICH TESTOSTERONE REPLACEMENT THERAPY?. Clinical Endocrinology, 21: 97-107


